Dr Huyam Salih, Director of AU-IBAR and Chair of the GF-TADs for Africa Regional Steering Committee (RSC). Picture (c) G. H. Bazimo (woah) 2024
This blog is an outcome of the third Standing Group of Experts’ (SGE) meeting on Contagious bovine pleuropneumonia (CBPP) in Africa, held online from 5 – 7 May 2025, under the aegis of the Africa chapter of the Global Framework for the progressive control of Transboundary Animal Disease (GF-TADs). An in-depth analysis of available date in WOAH’s World Animal Health Information System (WAHIS) provides insight into the distribution of the disease in Africa and the measures that countries (Members) have put in place to monitor the absence/presence or spread of this debilitating lung disease of cattle, caused by Mycoplasma mycoides subsp. mycoides (Mmm) (more information: Contagious bovine pleuropneumonia – WOAH). The disease is listed by WOAH and benefits from a WOAH official recognition of disease freedom pathway and from a WOAH endorsed official control programme for CBPP. Control options, in a nutshell, include vaccination, movement controls and/or stamping out (slaughter). Note that meat derived from stamping-out (test and slaughter) is nonetheless fit for human consumption and can be traded (Article.11.5.2 of the Terrestrial Animal Health Code on “Safe commodities”).
Out of the 54 Members of WOAH on the African continent (we excluded overseas territories such as St Helena, Réunion or Ceuta), 52 have reported on CBPP as either Absent or Present, including “Disease limited to one or more zones” or “Never reported” and/or “Suspected” (3)
The latest six-monthly reports (these can be six months away, or several years, depends on how timely countries report) point to 11 countries in which the disease is “Absent” and another 15 where the disease has “Never been reported”. This represents half of the countries that have
reported on CBPP to WOAH (26 out of 52) recently. All these data apply to domestic animals only, there is no known reservoir species of CBPP in wildlife.
Regardless of their status (disease present or absent) all countries should implement certain preventive and control measures, one of which is surveillance, the topic of the above mentioned third CBPP Standing Group of Experts (SGE) meeting in May 2025. For CBPP specifically there are up to 16 prevention, surveillance and control measures that apply (excluding e.g. vector control which is epidemiologically speaking irrelevant to CBPP), the maximum being reported by Members being 14.
The following measures could be regarded as part of the surveillance continuum, though others (e.g. movement control) are part of surveillance, and of control, depending on whether the disease is endemic or exotic) :
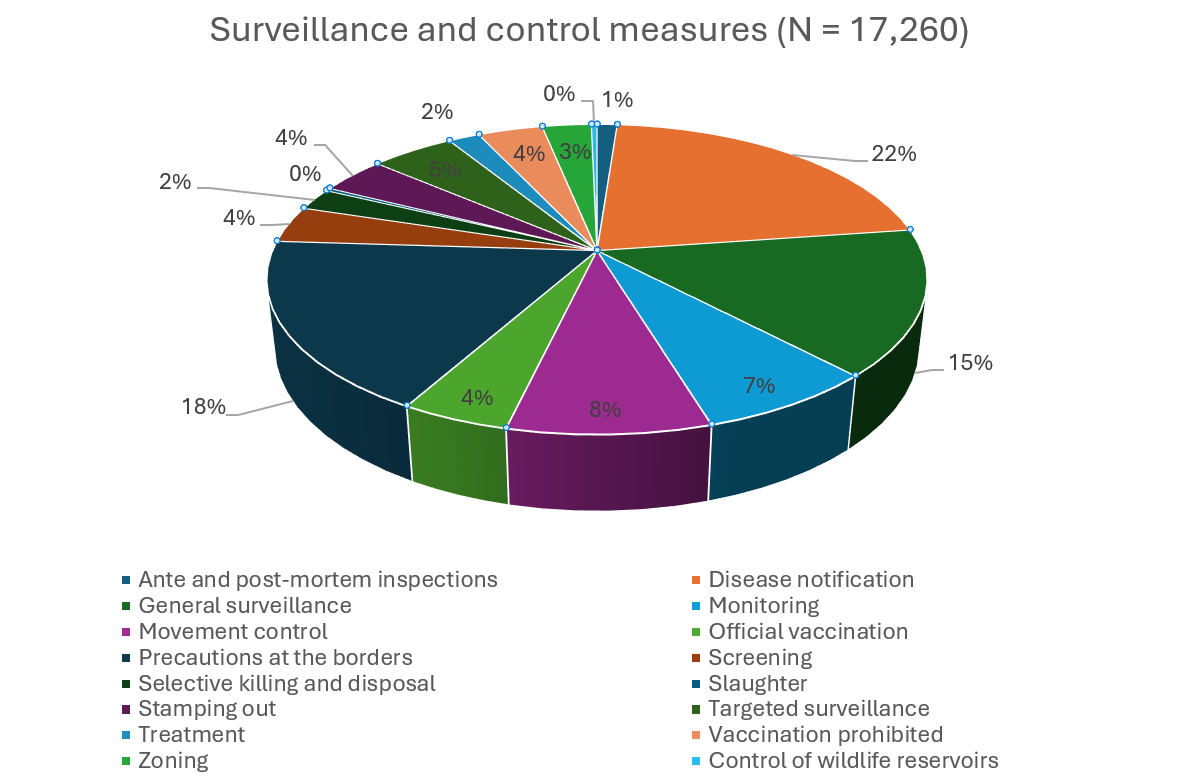
Based on 17,260 six-monthly reports submitted since 2005, the most reported measure is disease notification (22% of reports), followed by precautions at the borders (18%) and general surveillance (15%).
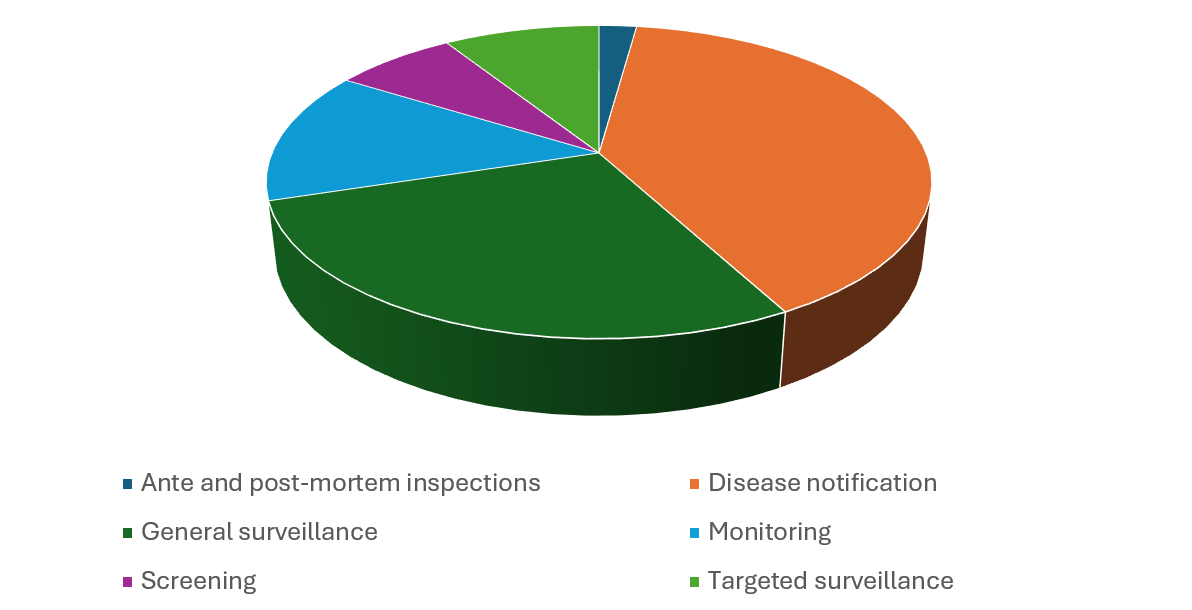
For these 17,260 records, surveillance and control measures are more or less balanced, 54% and 46% respectively, based on the above six surveillance measures chosen. For these six measures, the breakdown is as follows, with 40% reporting disease notification, 28% reporting general (passive) surveillance and 9% reporting targeted (active) surveillance.
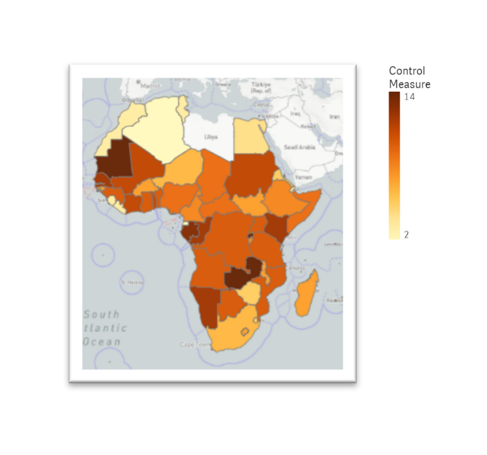
Further analysis focused on the question : are surveillance measures different between infected and non-infected countries ? To separate these two categories, we used the composite map on the right, which compiles all reports generated since the launch of WAHIS in 2005. Contrary to the previous map, it includes 32 countries (60%) that have reported the disease as present or suspected.
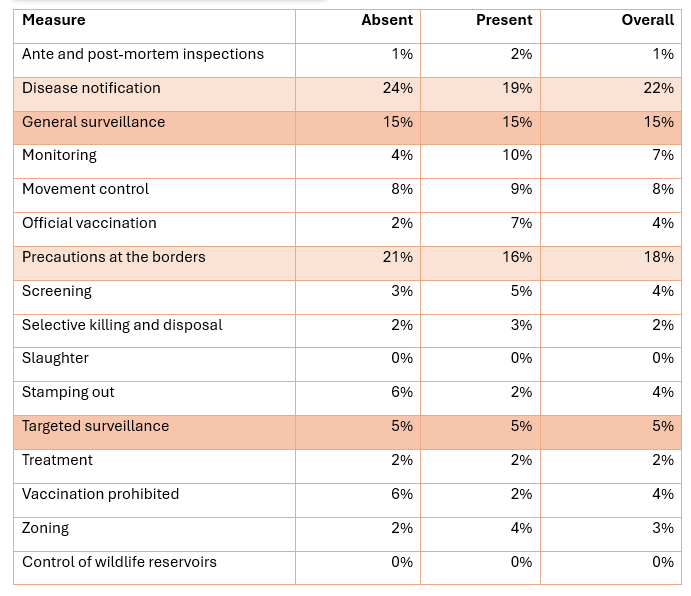
In the table below, we highlight notable differences in what is otherwise a similar attention to surveillance and control measures. This is the case for (again) disease notification and precautions at the borders, which -as expected- is higher in non-infected countries. Interestingly, both general surveillance and targeted surveillance are reported in exactly the same ration in both categories (15 and 5% respectively).
In conclusion, whilst 50% of Members in Africa have declared themselves as disease free in their latest six-monthly report the cumulative number of countries that are ‘very likely’ infected amount to 60% of countries, located in West, Central and Eastern Africa (the red ‘belt’ on the previous map). Note that only Botswana, eSwatini, Namibia (zone, south to the Veterinary Cordon Fence) and South Africa have been declared officially free from CBPP by WOAH. An extremely low percentage of countries (Members) report « ante and post-mortem inspections » as part of their surveillance measures whereas this is generally regarded as the most appropriate, sensitive and cost-effective tool in the surveillance toolbox. Is this because Members consider it part of general surveillance ? Or even targeted surveillance ? There seem to be no significant differences in the way disease-free countries design or regulate surveillance, except for a stronger focus on « disease notification » and border control.
Authors: Patrick Bastiaensen1, Viola Chemis2